The news on reproductive rights this year has not been good. Texas is shutting down health clinics, Ohio is forcing women to get an ultrasound before they get an abortion, Oklahoma is trying to restrict teens from buying Plan B over the counter—the country’s reproductive options are generally going to hell in a Republican handbasket.
But there’s one area of reproductive health that has been quietly and steadily improving for years: reducing teen pregnancies. During the last years of the Bush administration, the teen birth rate rose for the first time since 1992. But from 2007-2011 (the four most recent years the experts crunched the numbers), the trend swiftly reversed and the teen birth rate nationwide dropped a whopping 25 percent.
The reasons behind the drop are much more complex than just statistics on birth control use and funding for sex education—looking only at the dollars and data ignores the fact that we all learn about sex from the culture around us. Changing our most intimate behavior requires a major shift in the way governments and health-care experts engage with communities. While legislatures across the country have waged high-profile political battles over abortion politics, reproductive health advocates have made major progress under the radar by enabling women to control how and when they get pregnant in the first place.
In a country where reproductive-rights advocates are often too busy fighting political battles about pushing rights forward, the story of declining teen pregnancy rates is a case study in how the country can actually turn a worsening reality around. This article digs what’s behind the drop in just one state—Oregon—to illuminates what has changed about teen sex in the country as a whole over the past six years.
• • •

The Beaver State's teen birth rate decline is right in line with the national average, but in other reproductive rights areas, Oregon is at the top of a dismal heap. We’re the only state in the country that has not enacted any state-specific abortion restrictions post Roe v. Wade, and we’re one of only four states that meet even half the need for publicly funded birth control. Oregon is especially good at getting birth control to teens who need it; our state’s clinics meet 54 percent of teens’ contraceptive needs, bested only by Delaware, according to reproductive health research group the Guttmacher Institute’s 2010 Contraceptive Needs and Services study.
Right off the bat, it’s crucial to acknowledge that teen pregnancies are not an inherently bad thing. Teens who want to become pregnant should feel good about that choice, and discussions about teen birth rates shouldn’t revolve around making teens who get pregnant and raise kids feel bad about themselves. But teens are the group of Americans with the highest rate of unplanned pregnancies—in Oregon, 70 percent of teen pregnancies are unplanned—and so the recent steep drop in teen pregnancies means way more teens have gained the ability to avoid pregnancy if they want to. That should be the big goal of reproductive health work: not to shame or legislate people’s sex lives, but to help people control their bodies and choices, to equip all Americans with the resources and rights to live by their reproductive intentions—no matter who they are or which jerks control their statehouse.
That’s exactly what’s occurring in eight churches around Portland; community members are getting life lessons that would surprise right-wing Bible-beaters: sex-ed.
“We’re doing work that requires some really deep soul searching. That’s not really what health care is usually about,” says Mariotta Gary-Smith, Multnomah County’s African American Sexual Health Equity Program educator who coordinates an innovative program that trains African American Portlanders to lead sex-ed workshops in their own community spaces, including barbershops, hair salons, private homes, and places of worship.
“We encourage people to honor their faith, traditions, and beliefs,” Gary-Smith says. “We’re not there to demonize that. But we’re also encouraging people of faith to recognize that we live in the world and people have to make real-life decisions.”
The stats behind teen pregnancy don’t seem to make logical sense. Teens in Oregon are more sexually active than they were 10 years ago and they don’t seem to be getting any better at using contraception—yet rates of pregnancy, abortion, and birth have all declined. Every year, the state asks high schoolers to take a survey about their health and sexual activities. Since 2003, there’s been no pattern of change among contraceptive use, with about 17 percent of sexually active teens not using a reliable method. Meanwhile, more teens than a decade ago are having sex. There’s a reality here that the numbers miss.
Preventing pregnancy is not an equal playing field: Black and Latino teen girls are much more likely to have a child than white teens. In 2007, 27 out of every 1,000 white teen girls gave birth, compared to 46 black and 82 Latina girls between the ages of 15 and 19.

There are a couple hard numbers researchers can point to when explaining the demographic difference: the cost of birth control, for one, (without insurance, being on the pill can cost a woman up to $1,210 a year) and unequal access to health care depending on race and class.
But there's also a demographic difference in pregnancy reduction. In four years, the drop in pregnancy rates is startling, though race disparities remain. In 2011, 50 out of every 1,000 Latina teens ages 15-19 gave birth to a baby, compared to 34 black and 21 white. To help explain, local health workers have keyed in on differences in the lived experiences of people of color compared to white Portlanders.
Multnomah County Health Educator Molly Franks runs a federally funded program called Cuídate that leads eight-hour sexual health classes for Latino teens (350 teens last year, its first year of existence).
“I think in work on sexuality and health, it’s important that we talk about culture and I think we don’t often do it consciously. If we’re not doing it consciously, then we’re reflecting on the dominant culture, which is white. In this program, we call it out and talk about cultural values,” says Franks.
“One thing that is a big factor in the life of a lot of young people is that when they don’t see themselves being able to achieve things, like a career, having a child is a way to feel successful,” Franks continues. “Family is a really central value, being a parent is really important. That’s a success that’s accessible to people, when—because of racism and the economy—other avenues of success are not accessible to them.”
The Oregon education system also profoundly changed the way it approaches sex-ed—as of 2009, all Oregon schools are required to teach “medically accurate” sex-ed. That same year, the state put together an in-depth “Oregon Youth Sexual Health Plan” that’s surprisingly heartfelt and inspiring for a bureaucratic document. The plan lays out a mission statement for how state policies should support the sexual health of Oregon’s youth, and is built around an idea that sounds revolutionary in our current moralistic, finger-waving political landscape: “A holistic approach to sexual health supports physical, emotional, mental, and social well-being in relation to sexuality. As a result, the plan recognizes and advocates policies that help reduce poverty, discrimination, gender inequities and gender role expectations, and cultural assumptions of heterosexuality.”
Essentially, what health-care workers learned in the dark years between 2005 and 2007 was that just telling teens to abstain from sex was not an effective approach. Trying to reduce teen pregnancies by telling teens what not to do is myopic. As teenagers—especially black and Latino teens—start to grapple with issues of oppression, sex, and economics, they need support in developing healthy, empowered lives in general. Rather than telling teens what their sexual choices should be, they need the tools to decide for themselves.
“You can’t come into communities of color and say, ‘This is what needs to happen, so we’re going to do this,’” says health educator Gary-Smith, who works with Portland’s African American communities. “What you need to do instead is go to the community and have them determine what’s important to them, so it’s relevant to their lives. For communities that have a history of being disenfranchised and defined by others, giving them a space to talk about what that’s like for them—and then they can frame what they want—is really important.”
That grassroots approach to creating healthier sexual behavior is what led to the idea to train regular Portlanders to lead sex-ed discussions in black churches and community spaces.
“You’re reaching folks where they are,” says Gary-Smith.
This tactic is in line with the way our society has changed technologically—instead of having to rely on a single authority for information about sex (like a parent, teacher, or preacher), teens can now seek out sexual resources, conversations, and experiences online.
• • •
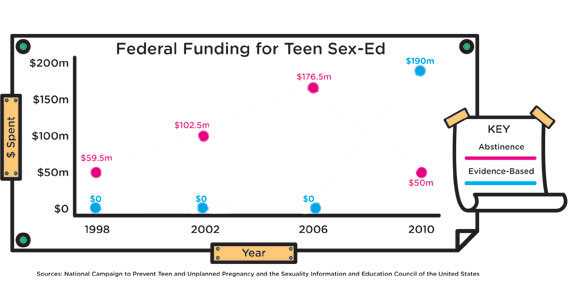
This local outreach and holistic work on sexual health is possible because of a major recent change in how the federal government funds sexual health programs. Instead of betting all its money on abstinence-only education, since 2010, reproductive health advocates pushed federal policy to instead favor “evidence-based” teen pregnancy prevention programs—meaning rigorous research has shown they’re actually effective.
Or, as Katy Suellentrop of the National Campaign to Prevent Teen and Unplanned Pregnancy puts it, “The biggest policy change in teen pregnancy was in 2010 when there was a focus on using programs that work.” From 1998 to 2010, the federal government spent over a billion dollars on abstinence-only sex education. During that same time, the teen birth rates slowed, flat-lined, then actually began to increase in 2006, and then declined again. Now, the government sets aside $190 million to fund “evidence-based” teen pregnancy prevention programs like the ones working with Multnomah County’s Latino youth.
While there’s more funding for sex-ed that actually works, other ways to prevent unplanned births have slipped behind. Like access to affordable birth control: It was actually harder to get birth control in 2010 than in 2001. According to the Guttmacher Institute's 2010 study, slightly more than half of women who wanted to use birth control in 2010 needed contraception that was subsidized or covered by public funds, because they were low income, lacked insurance, or both. While publicly funded clinics nationwide were able to meet 41 percent of the need for birth control in 2000, 10 years later they met only 35 percent. So while commentators of all political stripes bemoan the fact that nearly half of adult pregnancies are unplanned, millions of women are unable to get birth control that they need and want. This abysmal figure will (hopefully) improve thanks to Obamacare, which marks the one-year anniversary this month of its new rule that all insurance companies cover the entire cost of birth control for their clients (that’s right, ladies: all birth control types, no co-pay).
Conservatives often rail against the cost of paying for birth control, but preventing unplanned pregnancies is a sweet deal financially. According to 2010 data from the Guttmacher Institute, the annual public cost of contraception per-client is $239, while the public cost of each unplanned pregnancy is $12,770. Blue states are saving way more money than red states by preventing unwanted pregnancies—states that voted for Obama in 2012 save $5 billion annually by preventing unplanned pregnancies, nearly twice as much as states that vote Republican (who save $2.6 billion).

But if the major lesson to learn from the past five years of teen pregnancy prevention is that you can’t boil down why some teens get pregnant and some don’t to any single data point. The forces behind pregnancy rates are gigantic: the economy, politics, racism, our health-care system, family makeup, and religious values all play into how we talk about sex and with whom. Continuing to improve a single, simple outcome—reducing teen unplanned pregnancies—requires examining the complex roots of our behaviors, thinking of sexual health in a bigger way than lawmakers and educators ever have before, and literally taking the discussion to new places.
“We’re sitting inside people’s faith houses having real conversations about pregnancy and contraception and feelings and puberty,” says Gary-Smith, of her local program, which just got underway this year. “Having a conversation about condom use in the basement of a church is quite significant.”
This story made possible by a grant from the Quixote Foundation, as part of a joint project sponsored by the Media Consortium and the Association of Alternative Newsmedia. It is jointly published by The Portland Mercury and Bitch Media.
Graphs and illustrations by Bethany Ng.
Want the best of Bitch in your inbox? Sign up for our free weekly reader!